Perception of data quality and electronic health information system acceptance, reliability and satisfaction: A study at tertiary care hospital in Saudi Arabia
Electronic health information system: Data quality and user satisfaction
Revised : 2021-05-22
Accepted : 2021-05-30
Online : 2021-06-04
Print : 2021-06-05



Full text
Abstract
Electronic health information systems (EHIS) are considered a backbone for healthcare planning and quality services. This study was designed to explore the acceptance, reliability, and satisfaction of the end users' experience with the hospital electronic health information system. We also investigated the perception of data quality by the users who were directly involved in data entry. We conducted a questionnaire based cross-sectional survey to collect quantitative data from different EHIS users. The questionnaire contained six sections: demographic user information; general HIS assessment; accessibility and availability of computer terminals in the hospital; EHIS and the patient care; user satisfaction with the HIS and perception of data quality. Desktop computers were available throughout the hospital, but the hospital was lacking handheld computers or computers on wheels. Participants of the study were satisfied with the data entry and retrieval process but they were lacking job training related to troubleshooting. EHIS users were not aware and prepared for the downtime of the system and procedures were also not clear to them. Regarding the perception of data quality, most of the participants responded that data is of adequate quality. There is a need for proper technical support and enhance the hospital's networking speed for better response. Laptops and hand-held computers are the need of time for data entry in critical situations and during wards visit. This can also enhance the quality of data, and reduce the chances of data loss.
Keywords: Data quality, Electronic health information system (EHIS), Health information system (HIS), Implementation, Saudi Arabia, User satisfaction
How to cite: Mehmood A, Aqeeli AM, Musa A, Muhammad A, Muhammad O. Perception of data quality and electronic health information system acceptance, reliability and satisfaction: A study at tertiary care hospital in Saudi Arabia. Ann Med Physiol. 2021 Jan-Mar;5(1):1-6. doi: 10.23921/amp.2021v5i1.00044
Introduction
Innovative electronic health information systems (EHIS) are robust, automated, and advanced information systems for handling healthcare administrative, financial and clinical data. These significant systems play a vital role in documenting all aspects of patient care including medical services, evaluations, procedures, follow-up and critical medical decisions [1,2].
Health information systems can enhance health care provider efficiency by providing quality and cost savings healthcare services [3,4]. Different studies documented EHIS implementation and adaptation issues. The most reported issues were related to progress notes and other time-intensive components that forced medical professionals to spend extra time in data entry processes and exploring productive ways of using the EHIS [5,6]. This significant factor of time cost increased the resistance to use EHIS by physicians that undermines the potential for quality improvement [7]. IT firms are trying to boost EHIS usability by providing significantly advanced technology, such as voice recognition, tablet computers, wheel computers, or mobile hand-held devices. The development of user-friendly artificial intelligence (AI) based applications are a breakthrough in the medical industry that forced the software industry to think more censoriously about the application in healthcare domain [8].
During the implementation phase of electronic health information systems, most of the issues arise at the transition phase when healthcare professionals have to toggle between the paper base and electronic systems during the patient care process. This factor also slows down the workflow, takes more time to enter data from external systems manually and increases healthcare professionals' resistance to EHIS use [9]. Another issue during this phase is the inadequate electronic data exchange and integration between different EHIS modules and other electronic systems. Typically, EHIS systems need many difficult complimentary adjustments and support during the modification and final optimization procedure. EHIS developers, physicians and other healthcare professionals carry out several challenging and time-consuming practices to configure, adapt and augment the EHIS product until new technology benefits are achieved [6,9]. Electronic health information systems' development and implementation within the health system need coordination with data quality teams and end-users who directly interact with these systems [10,11].
Data quality is essential in planning and maintaining healthcare services. Indeed, structured quality data is the cornerstone of every healthcare organization [12,13].
King Fahd Central Hospital is also trying to implement the electronic health information system in all departments in full capacity and improving the data's reliability by enhancing the quality of data. The hospital is using an electronic health information system since 2015 in full capacity. Nevertheless, there are many challenges related to system usage, data quality, reliability, and integration.
We designed this study to explore the acceptance, reliability and satisfaction of the end users' experience with the electronic health information system. We also investigated the perception of data quality by the users who were directly involved in data entry.
Materials and methods
We performed this study from September 2020 to December 2020 at King Fahd Central Hospital, Jazan, Saudi Arabia. The study's targeted population was about 1606 hospital staff members. The participants were selected conveniently.
We conducted a cross-sectional survey and a questionnaire was adopted [14] to collect quantitative data from EHIS users. The questionnaire contained six sections: Demographic user information; General HIS assessment; Accessibility and availability of computer terminals in the hospital; EHIS and the patient care; User satisfaction with the EHIS and Perception of data quality attributes.
We distributed paper-based questionnaires to enhance the participants' responses and collected the filled responses within one week. The questionnaire was also translated into Arabic for better understanding among the participants. We circulated a total of 130 questionnaires among the heads of clinical departments, nursing supervisors, pharmacists, and administrative staff who was directly involved in supervision and data entry processes at outpatient clinics, wards and emergency departments. In response, we received 112 filled questionnaires from the participants as the remaining participants did not complete the questionnaire or were not available during the questionnaire collection period. Out of 112 filled and received questionnaires, 87 responses were found valid, while the others were incomplete.
Statistical analysis
We used the IBM SPSS version 25.0 to perform statistical analyses. Descriptive and inferential statistics were conducted. The significance was fixed at p<0.05.
Results
The total numbers of valid responses were 87, showing a response rate of 67%. The percentage of male and female participants was 59% and 41% respectively. The study's maximum participants were nurses (30%) and technicians (28%) who were using the health information system for data recording. The percentage and distribution of other participants are given in table 1. Most of the participants (40%) belong to the age group of 36-55 years, and 43% of participants had 2-5 years of job experience.
| Characteristics | Number | % | |
|---|---|---|---|
| Gender | Male | 51 | 59 |
| Female | 36 | 41 | |
| Age (years) | < 25 | 19 | 22 |
| 25-35 | 29 | 33 | |
| 36-55 | 35 | 40 | |
| > 55 | 4 | 5 | |
| Job category | Administration | 11 | 12 |
| Physician/Surgeon | 17 | 20 | |
| Pharmacists | 9 | 10 | |
| Nurses | 26 | 30 | |
| Technicians | 24 | 28 | |
| HIS experience in practice (years) | < 1 | 11 | 13 |
| 2-5 | 37 | 43 | |
| 5-8 | 13 | 15 | |
| > 8 | 26 | 30 | |
We applied the Chi square test to analyze the respondents' acceptance and satisfaction level towards the health information system.
Table 2 contains the results related to a general assessment of the Health information system, availability of computers at the health care facility, the performance of Health information systems, and the respondents' overall satisfaction level. We found that computers were available at the point of care and users were satisfied with the overall performance of the EHIS. Users agreed that the system is user friendly and help to improve patient care. According to the respondents, Laptops or computers on wheels were not available in the hospital. Overall, the users were satisfied with the EHIS performance but they were not agreed with the training facilities at the hospital.
| Characteristics | Strongly disagree | Disagree | Neutral | Agree | Strongly agree | *χ2 (p) | |
|---|---|---|---|---|---|---|---|
| *Chi-square test was not statistically significant if p-value more than the level of significance α=0.05 | |||||||
| HIS general assessment | HIS fonts and characters are easy to read | 0 | 14 | 49 | 24 | 0 | 163.31 (0.00) |
| HIS improves access to patient information | 0 | 0 | 36 | 49 | 2 | ||
| HIS is user friendly and easy to use | 0 | 2 | 42 | 41 | 2 | ||
| HIS performance speed is acceptable | 0 | 4 | 47 | 36 | 0 | ||
| HIS provides accurate information | 0 | 0 | 59 | 26 | 2 | ||
| HIS provides clear information | 0 | 7 | 56 | 24 | 0 | ||
| HIS provides sufficient information | 1 | 4 | 24 | 46 | 12 | ||
| HIS provides updated information | 2 | 4 | 34 | 43 | 4 | ||
| HIS screens layouts are appropriate | 3 | 12 | 47 | 22 | 3 | ||
| My practice needs are optimized by HIS | 0 | 2 | 25 | 54 | 6 | ||
| Availability of computer in hospital | Computer on wheels | 11 | 41 | 33 | 2 | 0 | 354.69 (0.00) |
| Computers are always available when I need them for HIS use | 0 | 20 | 47 | 20 | 0 | ||
| Desktop computers | 0 | 0 | 9 | 68 | 10 | ||
| Laptop computers | 49 | 29 | 9 | 0 | 0 | ||
| Patients care HIS performance | HIS improves the quality of patient care process | 0 | 2 | 41 | 44 | 0 | 122.63 (0.00) |
| HIS improves the quality of patient data entry and retrieval | 0 | 0 | 0 | 87 | 0 | ||
| Using HIS decreases time spent by patients inside hospital | 0 | 21 | 45 | 21 | 0 | ||
| User satisfaction | Current HIS training materials are helpful | 0 | 11 | 44 | 32 | 0 | 499.77 (0.00) |
| HIS downtime procedure is clear and comprehensive | 0 | 48 | 27 | 12 | 0 | ||
| I am prepared for HIS downtime | 0 | 28 | 50 | 9 | 0 | ||
| I am satisfied with the support provided to HIS users | 0 | 0 | 0 | 87 | 0 | ||
| I received enough training on HIS | 0 | 0 | 0 | 87 | 0 | ||
| Overall, I am satisfied with HIS | 0 | 0 | 87 | 0 | 0 | ||
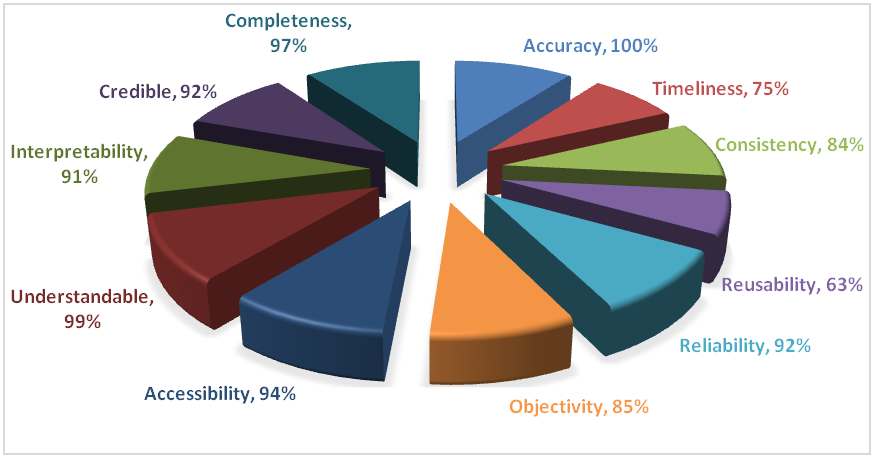
Figure 1 represents the participant's understanding of the data quality and its attributes. The 100% (87) of the participants responded that data is of appropriate quality, 97% (85) indicated that data must be complete, 99% (86) indicated that data must be understandable and meaningful, 91% (79) believed that data must be interpretable. In comparison, 94% (82) indicated that data must be accessible and traceable at the minimum time whenever required. All participants understand that the quality of data is essential and critical for any health care organization.
Discussion
We conducted this study to evaluate the acceptability and satisfaction level of the health information system (HIS). We had also taken the perception of participants regarding the data quality and reliability. For the development, implementation, and effective management of health information systems, health care professionals' engagement plays a critical role. It supports the health care organizations during and after the implementation process and feedback for its improvement. This engagement process can enhance the health information system's acceptability among health care professionals and the quality of data at the hospital.
The availability of computers on wheels was the least acceptable parameter, and participants were not satisfied with the unavailability of moveable computers and hand-held computers. Although the desktop computers were available at every department and point of contact, laptops and moveable computers were not available for immediate data entry or during the ward visit in a critical situation. Many studies also discussed the same issues in health care organizations where the moveable computers were not freely available [3,15,16].
The maintenance and downtime for system maintenance and system up-gradation were not defined and scheduled in the hospital. Sometimes the downtime was reported due to the internal network of the hospital. Participants were not fully satisfied with the system's speed and sometimes they had to spend much time during the data entry and retrieval process. This can also increase the waiting time of the patients. There was no alternative provided in the hospital that can be used during downtime or service disruption situations. The users had to maintain the manual record for the entry when the system was unavailable. Although the hospital is using third-party software that was responsible for its maintenance and troubleshooting; the management should have some checks for the smooth functioning of the system. This issue can have a serious impact on data quality and reliability, especially in critical situations. Many other studies have also pointed out this issue directly related to data quality, medication errors and incomplete data entry. They pointed out these issues in the outpatient settings while registering and admitting the patients at the hospital [15,17].
Overall, the study participants were satisfied with the electronic health information system's performance and acknowledged that this system helped in data standardization to some extent. Still, there is a need for improvement in the staff's training. Such type of training issues was also identified as a performance indicator in other studies [16,17].
In this study, we observed that the gender of participants did not affect satisfaction level. However, the years of HIS experience, job responsibility and age significantly affected the performance and HIS satisfaction level. Nurses and technicians were mostly satisfied with the HIS performance and found the system user friendly, while physicians’ response varied from neutral to satisfied as they were not ready to accept new technology that can delay or slow down the patient care process. Such type of technology adaptation hindrance and avoidance of electronic system evaluation for patient care were also highlighted in different studies [18,19].
Most of the participants were aware of data quality and its importance in a health care environment. As in this study, all participants agreed that accurate data is quality data. In contrast, 99% of the participants responded that the understandable data is quality, and 97% believed that complete data is quality data. We can compare our study results with the study conducted in Germany, where they found similar results regarding quality data perception [16,20,21].
Conclusions and recommendations
From the results and discussion of the study, we concluded that for quality data generation, acceptance and satisfaction of the health information system, it is essential to improve the EHIS efficiency and availability. In the hospital, there was lack of organizational support in terms of periodic training for the end users. Proper training can reduce patient waiting time and enhance work efficiency. There is a need for proper technical support from the vendor because most of the hospital uses third-party software and is dependent on them for software troubleshooting. The hospital is trying to upgrade the system from an application-based to a web-based system that will enhance the system's remote monitoring and enhance work efficiency.
There is a need to enhance the hospital's networking speed for better response. Laptops and hand-held computers are the need for data entry in critical situations and during wards visit. This can also enhance the quality of data, and there will be fewer chances of data loss.
Limitations
Due to limited time and resource constraints, the study was conducted in one hospital in the Jazan region of Saudi Arabia. Due to this limitation, it may not represent the other hospitals in the region or country. There is a need to explore further the perceptions on HIS software, data reliability and quality.
Declarations
Ethics approval and consent to participate
The ethical committee of Jazan University, Saudi Arabia, approved this study.
Acknowledgments
The authors would like to thank the Deanship of Scientific Research at Jazan University for the funding. We are also grateful to Director Quality Assurance and Mr. Abdu Mohammad Aqeeli (Statistician), King Fahd Hospital for providing support in data extraction and collection. Disclaimer: The contents are solely the responsibility of the authors and do not necessarily represent the official views of hospital management.
References
- Ismail A, Jamil AT, Rahman AF, Bakar JM, Saad NM, Saadi H. The implementation of hospital information system (HIS) in tertiary hospitals in Malaysia: A qualitative study. Malaysian Journal of Public Health Medicine. 2010;10(2):16-24.
- Shortliffe EH, Barnett GO. Biomedical data: Their acquisition, storage, and use. In: Shortliffe EH, Cimino JJ (eds). Biomedical informatics: Computer applications in health care and biomedicine. New York: Springer; 2006. p. 46-79. [Crossref]
- Ketikidis P, Dimitrovski T, Lazuras L, Bath PA. Acceptance of health information technology in health professionals: an application of the revised technology acceptance model. Health Informatics J. 2012 Jun;18(2):124-34. [Crossref] [Pubmed]
- World Health Organization. Everybody’s business: strengthening health systems to improve health outcomes: WHO’s framework for action. Geneva: World Health Organization; 2007. 44p.
- Pennington JW, Ruth B, Italia MJ, Miller J, Wrazien S, Loutrel JG, Crenshaw EB, White PS. Harvest: an open platform for developing web-based biomedical data discovery and reporting applications. J Am Med Inform Assoc. 2014 Mar-Apr;21(2):379-83. [Crossref] [Pubmed] [Pubmed Central]
- Denny JC. Chapter 13: Mining electronic health records in the genomics era. PLoS Comput Biol. 2012;8(12):e1002823. [Crossref] [Pubmed] [Pubmed Central]
- Ochieng OG, Hosoi R. Factors influencing diffusion of electronic medical records: a case study in three healthcare institutions in Japan. Health Inf Manag. 2006;34(4):120-9. [Crossref] [Pubmed]
- Hoffmann M, Loser K, Walter T, Herrmann T. A design process for embedding knowledge management in everyday work. In: Hayne SC, editor. Proceedings of the international ACM SIGGROUP conference on supporting group work - GROUP ’99; 1999 Nov 14-17; Phoenix, Arizona, USA. New York (NY): Association for Computing Machinery; 1999. 296-305. [Crossref]
- Lorenzi NM, Kouroubali A, Detmer DE, Bloomrosen M. How to successfully select and implement electronic health records (EHR) in small ambulatory practice settings. BMC Med Inform Decis Mak. 2009 Feb 23;9:15. [Crossref] [Pubmed] [Pubmed Central]
- Thompson TG, Brailer DJ (National Coordinator for Health Information Technology (ONCHIT)). The decade of health information technology: delivering consumer-centric and information-rich health care: Framework for strategic action. Washington, DC: US Department of Health and Human Services. 2004 Jul 21. 178p.
- Miller RH, Sim I, Newman J. Electronic medical records in solo/small groups: a qualitative study of physician user types. Stud Health Technol Inform. 2004;107(Pt 1):658-62. [Crossref] [Pubmed]
- Horvath MM, Rusincovitch SA, Brinson S, Shang HC, Evans S, Ferranti JM. Modular design, application architecture, and usage of a self-service model for enterprise data delivery: the Duke Enterprise Data Unified Content Explorer (DEDUCE). J Biomed Inform. 2014 Dec;52:231-42. [Crossref] [Pubmed] [Pubmed Central]
- Murphy SN, Gainer V, Chueh HC. A visual interface designed for novice users to find research patient cohorts in a large biomedical database. AMIA Annu Symp Proc. 2003;2003:489-93. [Pubmed] [Pubmed Central]
- Khalifa M, Alswailem O. Hospital information systems (HIS) acceptance and satisfaction: a case study of a tertiary care hospital. Procedia Computer Science. 2015;63:198-204. [Crossref]
- Berg M. Implementing information systems in health care organizations: myths and challenges. Int J Med Inform. 2001 Dec;64(2-3):143-56. [Crossref] [Pubmed]
- Atoyebi T. What are the barriers to E-coding of quality clinical data in irish hospitals from a coder’s perspective? [dissertation]. Dublin: University of Dublin; 2012. 123p.
- Chaudhry B, Wang J, Wu S, Maglione M, Mojica W, Roth E, Morton SC, Shekelle PG. Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med. 2006 May 16;144(10):742-52. [Crossref] [Pubmed]
- Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS quarterly. 1989 Sep 1; 13(3):319-40. [Crossref]
- Pai F, Huang K. Applying the technology acceptance model to the introduction of healthcare information systems. Technological Forecasting and Social Change. 2011 May;78(4):650-60. [Crossref]
- Britton JR. Healthcare reimbursement and quality improvement: integration using the electronic medical record comment on "Fee-for-service payment--an evil practice that must be stamped out?". Int J Health Policy Manag. 2015 May 8;4(8):549-51. [Crossref] [Pubmed] [Pubmed Central]
- Ancker JS, Kern LM, Abramson E, Kaushal R. The Triangle Model for evaluating the effect of health information technology on healthcare quality and safety. J Am Med Inform Assoc. 2012 Jan-Feb;19(1):61-5. [Crossref] [Pubmed] [Pubmed Central]