Prevalence of anemia in geriatric population of Kashmir: A hospital based study
Anemia: an unrecognised sign in geriatric patients
Revised: 2017-04-13
Accepted: 2017-04-13
Online: 2017-04-14
Print: 2017-04-30



Full text
Abstract
Anemia is a common concern in geriatric age group in developing countries. The purpose of this study was to identify the common causes and types of anemia in elderly patients in educationally backward region with limited access to quality health care. This was an observational study was done in Shri Maharaja Hari Singh (SMHS) Hospital of Government Medical College Srinagar, over a period of two years. 2000 patients above 60 years of age attending the outpatient clinic were screened for anemia based on WHO criteria. A random and non-consecutive selection of 100 anemic patients was done to study the morphological type and cause of anemia. 1160 (58%) patients were males and 840 (42%) were females. Total 812 out of 840 (96.67%) females and 738 out of 1160 (63.62%) males were found to be anemic. Maximum numbers of anemic patients were found in the age group 60-69 years. Mean age was 74.5 years. All the types of anemia based on peripheral smear were evident, normocytic being the commonest constituting 77.5%, followed by microcytic hypochromic 11.1%, macrocytic 7.05% and dimorphic 4.35%. 21% were lost to follow up and almost one fourth of the patients (24%) needed further evaluation before labelling them as having anemia due to old age. The common causes of anemia noted were gastrointestinal malignancy (31%), renal insufficiency (15%) and tuberculosis (9%). The inability to evaluate anemia in elderly individuals can lead to delay in the diagnosis of treatable as well as threatening disease conditions.
Keywords
Anemia, Gastrointestinal malignancies, Geriatric patients, Kashmir, Normocytic normochromic
Introduction
Anemia is a common concern in geriatric age group particularly in developing countries like India because of limited access to the quality healthcare, illiteracy and poverty. Anemia usually is not explained as an important sign to the geriatric patients in whom it is accepted as a result of aging process. Nevertheless, anemia in elderly should not be thought of merely as a result of aging [1]. According to WHO criteria, anemia is said to be present when the hemoglobin level is <13g/dl in a man and <12 g/dl in a woman [2]. Previous studies have shown that the prevalence of anemia increases as age advances. Below 75 years of age, it is found to be more common in female population, but above 75 years, it is more prevalent in males [2]. WHO data shows its prevalence to be between 8-44%; it being highest in men above 85 years of age [1]. In elderly population, anemia can have significantly more severe complications than in the younger adults and can greatly hamper the quality of life [3]. Studies have shown that anemia is an independent risk factor for increase in morbidity and mortality [4,5]. Stuides have also reported association between anemia and worsening of cognition and quality of life in elderly population [6,7]. Therefore anemia seems to have a significant effect on health indicators of a country and healthcare spending [8,9]. The present study has been undertaken to identify the common causes and types of anemia in elderly patients in educationally backward region with limited access to quality health care in Kashmir.
Materials and Methods
This was an observational study. A total of 2000 patients above 60 years of age attending the outpatient clinic in Shri Maharaja Hari Singh (SMHS) Hospital, Government Medical College Srinagar, over a period of two years, were screened for anemia based on WHO criteria [10] i.e. hemoglobin (Hb) <13 gm/dL in males and Hb <12 gm/dL in females. A random and non-consecutive selection of 100 anemic patients was done amongst the anemic population to study the morphological type of anemia and the common causes of anemia. Laboratory tests were done to fix the type of anemia. Types of anemia were classified based on RBC indices and further correlated by peripheral smear. The following hematological investigations were carried out for all patients: haemoglobin (Hb), total leucocyte count (TLC), differential leucocyte count (DLC), platelet count (PLT), reticulocyte count, erythrocyte sedimentation rate (ESR), packed cell volume (PCV), mean corpuscular volume (MCV), mean corpuscular hemoglobin concentration (MCHC), mean corpuscular hemoglobin (MCH) and peripheral smear for blood picture. Anemia was further classified based on MCV as microcytic (MCV <80fL), normocytic (MCV 80-100fL) and macrocytic (MCV >100fL). Dimorphic anemia was suspected when red cell distribution width (RDW) was more than its normal range (11-15%) and then correlated by peripheral smear. Such patients were further evaluated by fecal occult blood test (FOBT), upper and lower gastrointestinal endoscopy, renal function tests (blood urea, serum creatinine) and sputum examination or chest X ray (for tuberculosis) in suspected cases.
Results
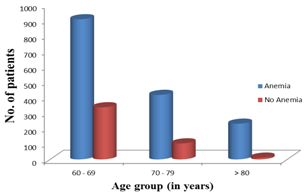
A total of 2000 patients were screened for the presence of anemia during the study period of two years. 1160 (58%) patients were males and 840 (42%) were females. The age distribution of the patients is shown in Table 1. Maximum numbers of subjects (1240) were in age group of 60-69 years, 519 in 71-79 years and 241 were in 80 years and above (Fig 1). Total 1550 out of 2000 (77.5%) patients were found to be anemic. 812 out of 840 (96.67%) females and 738 and 1160 (63.62%) males were found to be anemic amongst the study population. The subjects were further segregated according to age groups. Table 1 depicts that the prevalence of anemia increases as the age increases.
| Age (years) | Anemia | Total | Prevalence of anemia | |
|---|---|---|---|---|
| Present | Absent | |||
| 60-69 | 904 | 336 | 1240 | 72.9% |
| 70-79 | 416 | 103 | 519 | 80.2% |
| >80 | 230 | 11 | 241 | 95.4% |
| Total | 1550 | 450 | 2000 | |
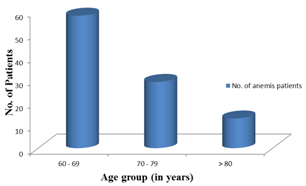
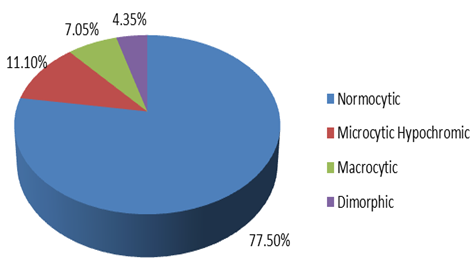
For knowing the type of anemia, a random selection of 100 patients was done from among the anemic subjects. The age distribution of these selected patients is depicted in Table 2 and Fig 2. Maximum numbers of anemic patients were found in the age group 60-69 years. Mean age for these selected patients was found to be 74.5. All the types of anemia based on peripheral smear were evident, normocytic being the commonest constituting 77.50%, followed by microcytic hypochromic 11.10%, macrocytic 7.05% and dimorphic 4.35% (Fig 3).
| Age group (years) | Number of anemic patients |
|---|---|
| 60-69 | 58 |
| 70-79 | 29 |
| >80 | 13 |
| Total | 100 |
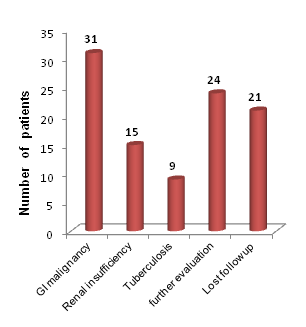
Among the 100 randomly selected patients, 31 patients had a GI malignancy. Fig 4 shows the common causes of anemia noted in our study.
Discussion
Though anemia in the elderly population is common, it is often attributed to be a consequence of aging process. Published literature has shown that advanced age is associated with low blood production accompanied with declining ratio of bone marrow to fat cells and lesser bone marrow response to erythropoietin stimulation [11]. This diminished response of bone marrow to erythropoietin is a key factor contributing to anemia in elderly along with reduced dietary intake and presence of comorbidities. Distinguishing anemia of chronic inflammation from anemia due to specific disease condition like chronic kidney disease (CKD) is challenging because chronic low-grade inflammation is seen in old age even without any known disease [12]. Evaluation and further course of management in younger adults is usually based on the mean corpuscular volume (MCV), however in elderly blood picture reveal normocytic, normochromic anemia. Therefore the treating physicians should have a degree of suspicion of underlying cause if routine hematological investigation and initial treatment is not successful [13]. Prevalence of anemia in old age in Kashmir is higher (77.5%) than reported by WHO report (2000) which was about 50% in developing countries and 12% in developed countries [14]. In our study percentage of anemia in males was less as compared to females in contrast to Guralink et al [15] and NHANES-III study of World Health Organization both of which showed higher prevalence of anemia in men than in women [14]. These gender differences noted in our study can be attributed to the traditional customs and old beliefs of avoiding several food commodities in elderly age. However our results corroborate with the Nissenson et al [16] study which also revealed a higher prevalence of anemia in females (20%) than in males (7.5%).
Most common morphological type of anemia in the present study was normocytic anemia accounting for 77.5%. These findings corroborate closely with Kim and Lee [17] and Choi et al [18] who found normocytic anemia amounting to 93.5%, microcytic anemia 3.5% and macrocytic anemia to be 3%. Elis et al have also shown that most common anemia in elderly is normocytic normochromic type [19].
While a significant proportion of patients in our study (21%) were lost to follow up and one fourth of the patients (24%) needed further evaluation before labelling them as having anemia due to old age. We found that significant number of the patients (31%), on further investigations, were found to be harbouring a gastrointestinal (GI) malignancy which is an alarming concern for healthcare system to look into the risk factors for higher predisposition to malignancy in geriatric age group in Kashmir with anemia as a common presentation which is usually ignored as unimportant condition in advanced age leading to delay in seeking medical help.
Limitations of the study
Most important reason for higher prevalence of anemia in the current study is that ours was a hospital based study as compared to the other studies which were population based studies.
Conclusion
We conclude that anemia is highly prevalent in aged individuals. Failure to evaluate anemia in elderly could lead to delayed diagnosis of treatable sinister conditions and also progression and advancement of potentially life threatening conditions like malignancies. Confirming the type of anemia is vital to focus on the investigations for identifying the etiology. Nonspecific symptoms like easy fatigability and general weakness should not be ignored in the geriatric population as just senile symptoms because they could be important indicators of presence of anemia and its underlying cause which warrants a thorough evaluation.
Suggestion
We suggest that a general awareness campaign be launched, so as to make the people aware of the importance of anemia in elderly age seeking early medical advice. Anemia in elderly should not merely be considered as "normal aging" process and blanket treatment with hematinics should be avoided. A governmental initiative to emphasize the need of creating awareness in the society about the importance of anemia in geriatric age group might be a cost-effective modality in terms of early diagnosis and treatment.
Acknowledgments
None.
Source of funding
None
References
- World Health Organization. Definition of an older or elderly person. Available at http://www.who.int/healthinfo/survey/ageingdefnolder/en/index.html [Last accessed August 29, 2010]
- Ferrucci L, Semba RD, Guralnik JM, Ershler WB, Bandinelli S, Patel KV, Sun K, Woodman RC, Andrews NC, Cotter RJ, Ganz T, Nemeth E, Longo DL. Proinflammatory state, hepcidin and anemia in older persons. Blood. 2010 May 6; 115(18):3810-6. [Pubmed] [Crossref]
- Bhasin A, Rao MY. Characteristics of anemia in elderly: a hospital based study in South India. Indian J Haematol Blood Transfus. 2011 Mar; 27(1): 26-32. [Pubmed] [Crossref]
- Chaves PH, Ashar B, Guralnik JM, Fried LP. Looking at the relationship between hemoglobin concentration and prevalent mobility difficulty in older women. Should the criteria currently used to define anemia in older people be reevaluated? J Am Geriatr Soc. 2002 Jul; 50(7):1527-64. [Pubmed] [Crossref]
- Beattie WS, Karkouti K, Wijeysundera DN, Tait G. Risk associated with preoperative anemia in noncardiac surgery: a single-center cohort study. Anesthesiology. 2009 Mar; 110(3):574-81. [Pubmed] [Crossref]
- Lucca U, Tettamanti M, Mosconi P, Apolone G, Gandini F, Nobili A, Tallone MV, Detoma P, Giacomin A, Clerico M, Tempia P, Guala A, Fasolo G, Riva E. Association of mild anemia with cognitive, functional, mood and quality of life outcomes in the elderly: the “Health and Anemia” study. PloS One. 2008 Apr 2; 3(4):e1920. [Pubmed] [Crossref]
- Riva E, Tettamanti M, Mosconi P, Apolone G, Gandini F, Nobili A, Tallone MV, Detoma P, Giacomin A, Clerico M, Tempia P, Guala A, Fasolo G, Lucca U. Association of mild anemia with hospitalization and mortality in the elderly: the Health and Anemia population-based study. Haematologica. 2009 Jan; 94(1):22-8. [Pubmed] [Crossref]
- Robinson B. Cost of anemia in the elderly. J Am Geriatr Soc. 2003 Mar; 51(3 suppl):S14-7. [Pubmed] [Crossref]
- Ershler WB, Chen K, Reyes EB, Dubois R. Economic burden of patients with anemia in selected diseases. Value Health. 2005 Nov-Dec; 8(6):629-38. [Pubmed] [Crossref]
- World Health Organization. Nutritional anaemias. Report of a WHO scientific group. WHO Technical Report Series No 405. World Health Organ Tech Rep Ser. 1968; 405:5-37. [Pubmed]
- Mehta BC. Iron deficiency anemia. In: Shah SN (ed). API Textbook of Medicine, 7th ed. Association of Physicians of India, Mumbai, pp.930-4, 2003.
- Beutler E, Waalen J. The definition of anemia: what is the lower limit of normal of the blood hemoglobin concentration? Blood. 2006 Mar; 107(5):1747-50. [Pubmed] [Crossref]
- Chaves PH, Xue QL, Guralnik JM, Ferrucci L, Volpato S, Fried LP. What constitutes normal hemoglobin concentration in community-dwelling disabled older women? J Am Geriatr Soc. 2004 Nov; 52(11):1811-6. [Pubmed] [Crossref]
- Chernetsky A, Sofer O, Rafael C, Ben-Israel J. Prevalence and etiology of anemia in an institutionalized geriartic Harefuah 2002 Jul; 141(7):591-4. [Article in Hebrew] [Pubmed]
- Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC. Prevalence of anemia in persons65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood. 2004 Oct 15; 104(8):2263-8. [Pubmed] [Crossref]
- Nissenson AR, Goodnough LT, Dubois RW. Anemia: not just an innocent by stander? Arch Intern Med 2003 Jun 23; 163(12):1400-4. [Pubmed] [Crossref]
- Kim HS, Lee BK. Cross-sectional study on the prevalence of anemia among rural elderly in Asan. Nutr Res Pract 2008 Spring; 2(1):8-12. [Pubmed] [Crossref]
- Choi CW, Lee J, Park KH, Yoon SY, Choi IK, Oh SC, Seo JH, Kim BS, Shin SW, Kim YH, Kim JS. Prevalence and characteristics of anemia in the elderly: cross-sectional study of three urban Korean population samples. Am J Hematol. 2004 Sep; 77(1):26-30. [Pubmed] [Crossref]
- Elis A, Ravid M, Manor Y, Bental T, Lishner M. A clinical approach to “idiopathic” normocytic-normochromic anemia. J Am Geriatr Soc. 1996 Jul; 44(7):832-4. [Pubmed] [Crossref]